For Health Priorities in Australia, one of the first issues you are asked to consider is how we identify priority issues for Australia’s health? This question is almost identical to the critical question “How are priority issues for Australia’s health identified?”
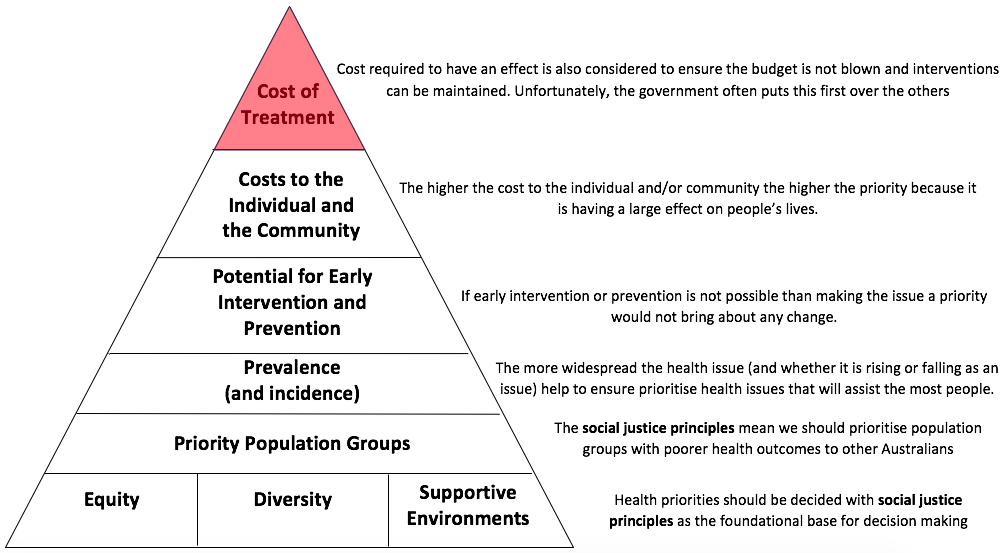
The principles of social justice, as covered in Preliminary PDHPE (see here), are: equity, diversity, and supportive environments, and are the foundation for identifying priority health issues in Australia. This means that providing non-equal, but equitable distribution of resources so that all Australians are more able to reach the same levels of health. It means the differences between individuals and people groups are considered and either addressed, if differences in health outcomes, or considered in how health is promoted. It also means that the government and other bodies consider the environment people live in and its effect on health outcomes.
One of the results of the principles of social justice is that various people groups are examined and considered when identifying priority health issues. This is seen in reports such as Australia’s Health 2016, where groups such as our indigenous people, people living in rural and remote areas, or those who live with a disability. These groups are considered individually to identify health issues that are specific to the group because epidemiology tells us they have lower levels of health than other Australians. Therefore, the government applied the principles of equity to provide greater resources to these groups to improve their health and seeks to create an environment to support such groups to achieve better health outcomes.
The prevalence of the condition is also considered in identifying priority health issues in Australia. This is the more obvious criteria to use. There is no point making an issue a priority if it only affects a very small number of people. If the issue is prevalent, however, it needs to become a priority so that the health of more people is improved by addressing the one issue. This has been seen over the last few decades as smoking rates have been targetted in Australia to help reduce the incidence of cardiovascular disease.
Another key consideration in identifying priority health issues is the potential for early intervention and/or prevention. If a health issue can be prevented through changes in lifestyle, then health promotion in this area is likely to improve outcomes, as a change in lifestyle may prevent the disease altogether. For example, improving your diet and doing exercise can help reduce the likelihood of getting CVD, diabetes and many other diseases. This is similar to early intervention. Diseases such as cancer, also have better survival rates if the cancer is found early and treated early, therefore early intervention can help to improve health outcomes and so it is more likely to become a health priority.
The final consideration is the cost to the individual and the community. Some diseases have a large cost for the individual and community, while other have a very small cost. If we consider musculoskeletal injuries, some injuries such as a spinal injury, have large ramifications. The person may become a paraplegic and have to stop working, change jobs, renovate or move house and much more. It may put a strain on their relationships, decrease their social, mental, emotional, and spiritual health with the physical condition. The cost is high to both the individual and the community. On the other hand, a sprained ankle may mean you have to take a day or 2 off work and use crutches for a while, but you will recover quickly and the cost will be fairly minor. So although the incidence and prevalence of a sprained ankle are much higher, it does not become a health priority.
To conclude, it is worth noting that in reality, the main people in charge of identifying health priorities in Australia are influenced by much more than these considerations. Lobbying bodies and the media will also try and influence decisions around health priorities in Australia, but the more influential groups are those who make money from the health industry and the government’s budget. Of particular concern is the influence the drug companies have on the government. These companies make drugs such as pain killers, antibiotics, and vaccines. If they can convince the government, for example, to make a disease they have a vaccine for a health priority, the government then rolls out the new vaccine to every child in Australia and the company makes $billions. Furthermore, in order to do this, the government has to get the money from somewhere to pay for it. This means either shifting money around within health care, such as removing hospital funding, or moving it from other priorities such as industrial development, or even increasing taxes.
Often the government does not prioritise particular health issues because of the cost of treatment, or prevention. Governments want to stay in office, so avoid increasing taxes as much as possible. But this can result in some issues that should be prioritised being overlooked, and not funded. So although the HSC PDHPE syllabus correctly identifies how health issues are identified, this does not mean the bodies responsible for health respond to the priorities as they should.